Work package 3
WP3: Epidemiology: Risk factors of diabetic neuropathy in type 2 diabetes
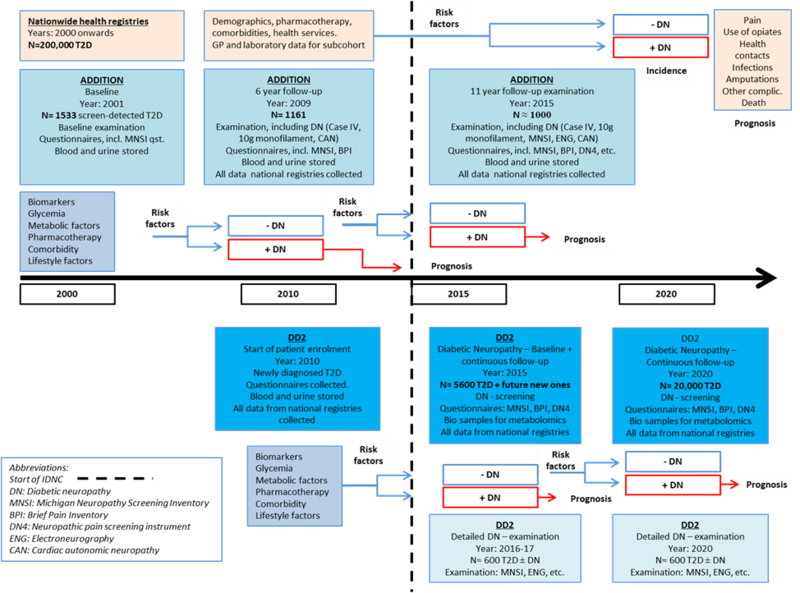
The overall hypothesis in this work package is that factors other than hyperglycaemia represent important, potentially modifiable, risk and prognostic factors for diabetic neuropathy in type 2 diabetes. We will exploit the ADDITION Denmark cohort and the DD2 cohort to clarify a) metabolic risk factors for diabetic neuropathy, b) existing therapy effects against diabetic neuropathy, and c) determinants of the clinical course and prognosis of diabetic neuropathy. In a), we will examine whether the risk of nerve injury is primarily related to the underlying glucose control, blood pressure control, or lipid control. In b), we will examine if several existing drug therapies for diabetes have a beneficial effect for the prevention and treatment of diabetic neuropathy. To overcome expected problems with confounding by indication and time-varying confounders, we will apply advanced statistical approaches. In c), we will further clarify the natural history of patients with diabetic neuropathy including the impact of patient-oriented outcomes. Specifically, we will examine the biological interaction and impact of antidiabetic therapies, glycaemic and lipid control, and lifestyle factors on clinical diabetic neuropathy outcomes to form the basis for future intervention studies. Finally, we will evaluate the prognostic effect of diabetic neuropathy per se in type 2 diabetes. This plan will be achieved by integrating data from the cohorts described in WP3.1, WP3.2, and WP3.3. Please see also the summary diagram of this work package.
WP3.1
In the prospective ADDITION cohort study and biobank starting in 2001, a screening program in Danish general practices identified 1,533 patients with type 2 diabetes and they continue to be followed. Patients were examined at baseline and at 6-year follow-up, and blood and urine samples were collected. The presence of diabetic neuropathy was assessed at 6 years with the following measures: vibration detection threshold, light touch sensory testing, Michigan Neuropathy Screening Inventory (MNSI), and the Brief Pain Inventory (BPI). The presence of cardiac autonomic neuropathy was assessed using heart rate variability at supine rest and three standard tests (Valsalva, deep breathing, and standing). In this program, patients will be re-examined using the above-mentioned tests and a series of other tests. This will allow us to perform a longitudinal study, investigating the association between changes in metabolic and other risk factors over time and the development of diabetic neuropathy over a 15-year period.
WP3.2
In the prospective DD2 cohort and biobank, newly diagnosed type 2 diabetes patients throughout Denmark will be enrolled. The DD2 currently enrolls 60 new T2D patients per week and currently holds more than 7,952 incident type 2 diabetes patients with biobank data (www.dd2.nu). The DD2 cohort will become 10 times larger than the ADDITION cohort within the next few years and offers the possibility of enrolling new type 2 diabetes patients for detailed diabetic neuropathy examinations. A sample will be invited for a more detailed diabetic neuropathy examination. These more specific measures will allow for a well-characterised cohort meeting a stringent definition and classification of diabetic neuropathy. This cohort will form the basis of a cross-sectional analysis and in time a prospective analysis of risk factors for diabetic neuropathy. A subset of samples from this cohort will be sent to the Feldman Lab for targeted metabolomics analysis. Finally, patients examined in the DD2 will be used to validate register-based information on diabetic neuropathy.
WP3.3
In the nationwide Danish healthcare registries, almost the entire Danish population with diabetes (currently ~320,000) can be identified through validated algorithms, linking hospital contacts, prescriptions, health services, and e-data from general practitioners. We will validate hospital discharge, outpatient clinic, and general practitioner diagnoses of diabetic neuropathy by medical record review and linkage with the ADDITION and DD2 cohorts, respectively. We will exploit these large nationwide data sources to test hypotheses on glycaemia, pharmacotherapy, and comorbidity on a national level. We will also obtain up-to-date estimates on incidence, prevalence, and time trends of DN and its complications in Denmark.